Therapeutic Classification: CYTOSTATIC AGENT (L: antineoplastic and immunomodulating agents-platinum compounds).
ATC Code: L01XA03.
Pharmacology: Pharmacodynamics: Oxaliplatin is an antineoplastic drug belonging to a new class of platinum-based compounds in which the platinum atom is complexed with 1,2-diaminocyclohexane ("DACH") and an oxalate group.
Oxaliplatin is a single enantiomer, the Cis-[oxalato(trans-l-1,2- DACH)platinum].
Oxaliplatin exhibits a wide spectrum of both in vitro cytotoxicity and in vivo antitumour activity in a variety of tumour model systems including human colorectal cancer models. Oxaliplatin also demonstrates in vitro and in vivo activity in various cisplatin resistant models.
A synergistic cytotoxic action has been observed in combination with 5-fluorouracil both in vitro and in vivo.
Studies on the mechanism of action of oxaliplatin, although not completely elucidated, show that the aqua-derivatives resulting from the biotransformation of oxaliplatin, interact with DNA to form both inter and intra-strand cross-links, resulting in the disruption of DNA synthesis leading to cytotoxic and antitumour effects.
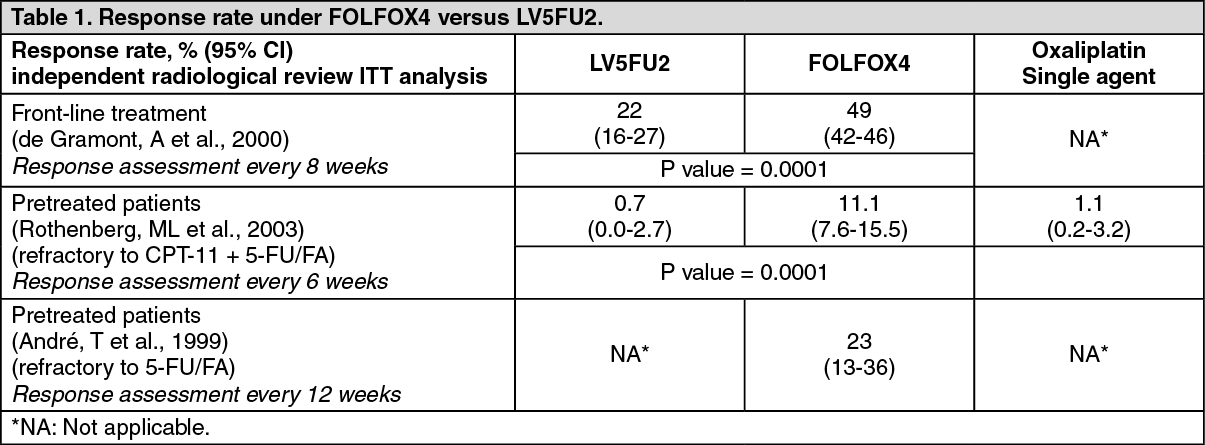
In patients with metastatic colorectal cancer, the efficacy of oxaliplatin (85mg/m
2 repeated every two weeks) combined with 5-fluorouracil/folinic acid (5-FU/FA) is reported in three clinical studies: In front-line treatment, a 2-arm comparative phase III study (de Gramont, A et al., 2000) randomised 420 patients either to 5-FU/FA alone (LV5FU2, N=210) or the combination of oxaliplatin with 5-FU/FA (FOLFOX4, N=210).
In pretreated patients, a comparative three arms phase III study (Rothenberg, ML et al., 2003) randomised 821 patients refractory to an irinotecan (CPT-11) + 5-FU/FA combination either to 5-FU/FA alone (LV5FU2, N=275), oxaliplatin single agent (N=275), or combination of oxaliplatin with 5-FU/FA (FOLFOX4, N=271).
Finally, an uncontrolled phase II study (André, T et al., 1999) included patients refractory to 5-FU/FA alone, that were treated with the oxaliplatin and 5-FU/FA combination (FOLFOX4, N=57).
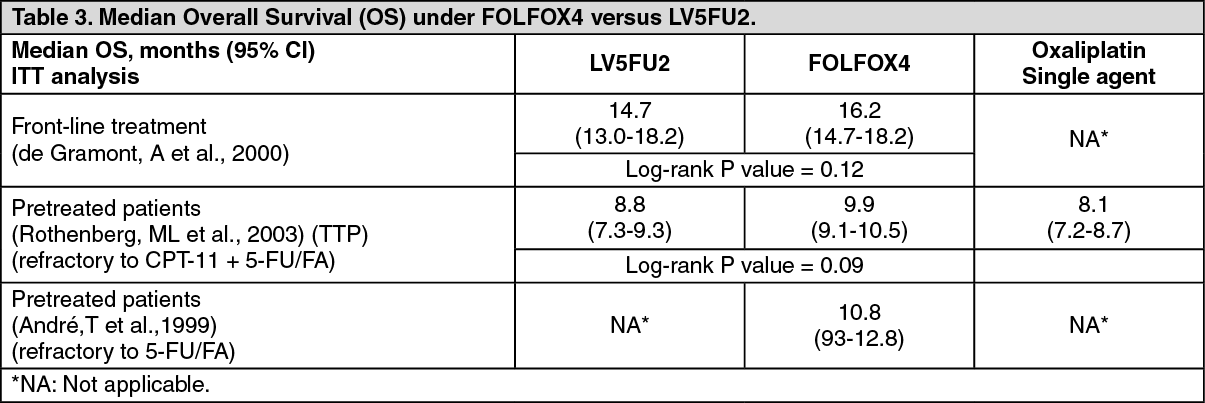
The two randomised clinical trials in front-line therapy (de Gramont, A et al.) and in pretreated patients (Rothenberg ML et al.), demonstrated a significantly higher response rate and a prolonged progression free survival (PFS)/time to progression (TTP) as compared to treatment with 5-FU/FA alone. ln the study of Rothenberg et al. performed in refractory pretreated patients, the difference in median overall survival (OS) between the combination of oxaliplatin and 5-FU/FA versus 5-FU/FA did not reach statistical significance. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In pretreated patients (Rothenberg, ML et al., 2003), who were symptomatic at baseline, a higher proportion of those treated with oxaliplatin and 5-FU/FA experienced a significant improvement of their disease-related symptoms compared to those treated with 5-FU/FA alone (27.7% vs 14.6%, p=0.0033).
In non pretreated patients (de Gramont, A et al., 2000), no statistically significant difference between the two treatment groups was found for any of the quality of life dimensions. However, the quality of life scores were generally better in the control arm for measurement of global health status and pain and worse in the oxaliplatin arm for nausea and vomiting.
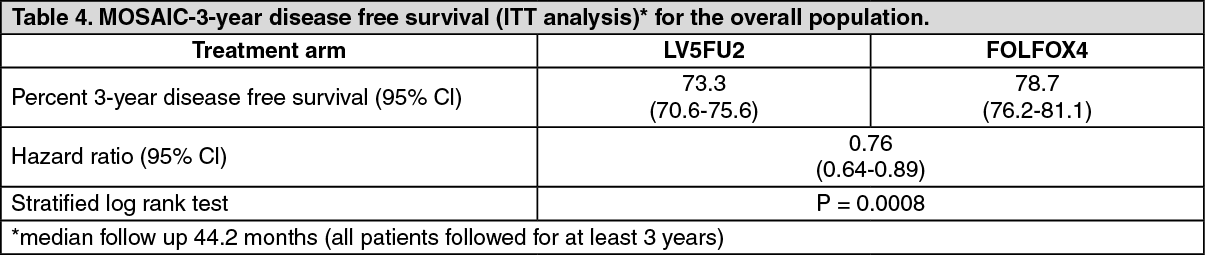
In the adjuvant setting, the MOSAIC comparative phase III study randomised 2246 patients (899 stage II / Duke's B2 and 1347 stage III / Duke's C) further to complete resection of the primary tumor of colon cancer either to 5-FU/FA alone (LV5FU2, N=1123 (B2 / C = 448 / 675) or to combination of oxaliplatin and 5-FU/FA (FOLFOX4, N=1123 (B2 / C) = 451 / 672). (See Table 4.)
Click on icon to see table/diagram/image
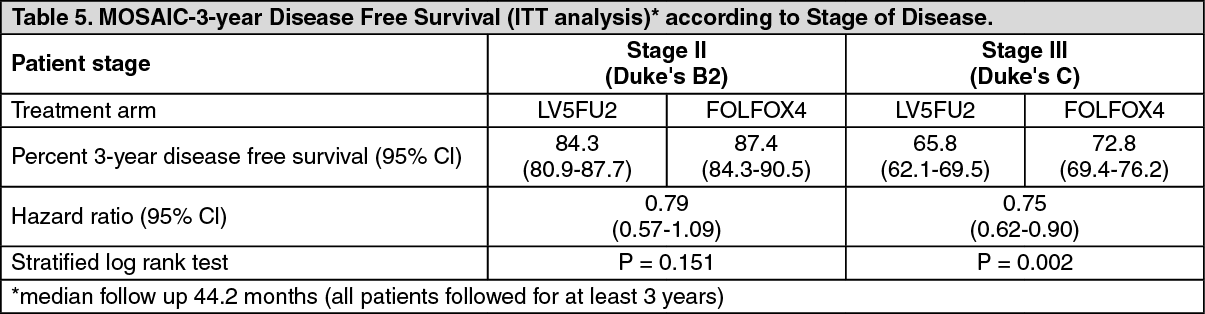
The study demonstrated an overall significant advantage in 3-year disease free survival for the oxaliplatin and 5-FU/FA combination (FOLFOX4) over 5-FU/FA alone (LV5FU2). (see Table 5.)
Click on icon to see table/diagram/image
Overall Survival (ITT analysis): At time of the analysis of the 3-year disease free survival, which was the primary endpoint of the MOSAIC trial, 85.1% of the patients were still alive in the FOLFOX4 arm versus 83.8% in the LV5FU2 arm. This translated into an overall reduction in mortality risk of 10% in favour of FOLFOX4 not reaching statistical significance (hazard ratio = 0.90). The figures were 92.2% versus 92.4% in the stage II (Duke's B2) sub-population (hazard ratio = 1.01) and 80.4% versus 78.1% in the stage III (Duke's C) sub-population (hazard ratio = 0.87), for FOLFOX4 and LV5FU2, respectively.
Pharmacokinetics: The pharmacokinetics of individual active compounds have not been determined. The pharmacokinetics of ultrafiltrable platinum, representing a mixture of all unbound, active and inactive platinum species, following a two-hour infusion of oxaliplatin at 130mg/m
2 every three weeks for 1 to 5 cycles and oxaliplatin at 85mg/m
2 every two weeks for 1 to 3 cycles are as follows: see Table 6.
Click on icon to see table/diagram/image
At the end of a 2-hour infusion, 15% of the administered platinum is present in the systemic circulation, the remaining 85% being rapidly distributed into tissues or eliminated in the urine. Irreversible binding to red blood cells and plasma, results in half-lives in these matrices that are close to the natural turnover of red blood cells and serum albumin. No accumulation was observed in plasma ultrafiltrate following 85mg/m
2 every two weeks or 130mg/m
2 every three weeks and steady state was attained by cycle one in this matrix. lnter- and intra-subject variability is generally low.
Biotransformation in vitro is considered to be the result of non-enzymatic degradation and there is no evidence of cytochrome P450-mediated metabolism of the diaminocyclohexane (DACH) ring.
Oxaliplatin undergoes extensive biotransformation in patients, and no intact drug was detectable in plasma ultrafiltrate at the end of a 2h-infusion. Several cytotoxic biotransformation products including the monochloro-, dichloro- and diaquo-DACH platinum species have been identified in the systemic circulation together with a number of inactive conjugates at later time points.
Platinum is predominantly excreted in urine, with clearance mainly in the 48 hours following administration.
By day 5, approximately 54% of the total dose was recovered in the urine and < 3% in the faeces.
A significant decrease in clearance from 17.6 ± 2.18 l/h to 9.95 ± 1.91 l/h in renal impairment was observed together with a statistically significant decrease in distribution volume from 330 ± 40.9 to 241 ± 36.1 l. The effect of severe renal impairment on platinum clearance has not been evaluated.
Toxicology: Preclinical safety data: The target organs identified in preclinical species (mice, rats, dogs, and/or monkeys) in single- and multiple-dose studies included the bone marrow, the gastrointestinal system, the kidney, the testes, the nervous system, and the heart. The target organ toxicities observed in animals are consistent with those produced by other platinum-containing drugs and DNA-damaging, cytotoxic drugs used in the treatment of human cancers with the exception of the effects produced on the heart. Effects on the heart were observed only in the dog and included electrophysiological disturbances with lethal ventricular fibrillation. Cardiotoxicity is considered specific to the dog not only because it was observed in the dog alone but also because doses similar to those producing lethal cardiotoxicity in dogs (150mg/m
2) were well-tolerated by humans. Preclinical studies using rat sensory neurons suggest that the acute neurosensory symptoms related to Oxaliplatin may involve an interaction with voltage-gated Na+ channels.
Oxaliplatin was mutagenic and clastogenic in mammalian test systems and produced embryo-fetal toxicity in rats. Oxaliplatin is considered a probable carcinogen, although carcinogenic studies have not been conducted.



 Sign Out
Sign Out